
.jpg)
Case Series/Study
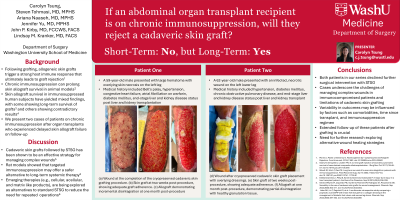
A 59-year-old male with end-stage renal (ESRD) and liver disease (ESLD), chronic anemia, atrial fibrillation, hypertension, and liver/kidney transplantation 3 months prior presented with a large hematoma with overlying skin necrosis. Following debridement, a 25 x 9 cm cadaveric skin graft was applied to the lower left extremity wound with concurrent negative pressure wound therapy. Postoperatively, the patient’s immunosuppressive therapy was continued. The allograft demonstrated initial adherence but ultimately failed within 19 weeks. The patient was offered an elective STSG but preferred to continue with local wound care.
A 62-year-old male with a history of ESLD , ESRD secondary to diabetes/hypertension, and combined liver/kidney transplant 6 years prior presented with a left leg necrotizing soft tissue infection. After serial debridements, he received a 24 x 10 cm cadaveric skin graft and was continued on an appropriate immunosuppression regimen postoperatively. The graft initially adhered successfully but ultimately failed after 11 weeks. The patient was offered an elective STSG but declined in favor of local wound care.