(CR-003) A Comprehensive Approach to Pressure Injury Management via Multimodal Wound Imaging and What Is Next in Pressure Injury Prevention
Friday, May 2, 2025
7:45 PM - 8:45 PM East Coast USA Time
Katherine McLeod, RN
Introduction: Pressure injuries pose a significant economic burden on U.S. hospitals and healthcare facilities, leading to higher treatment costs, extended hospital stays, and increased liability risks. Effective prevention and management are essential to reduce these financial and legal challenges. This study examines the outcomes of a multimodal approach to the prevention and management of pressure injuries (PIs), integrating clinical standard of care (SOC) assessment, bacterial fluorescence (FL) imaging, and the addition of thermal imaging for detecting deep tissue injuries (DTI) as a preventive strategy, all facilitated by a single imaging device.
Methods: Three data sources involving a single wound imaging device* were utilized in this study. First, the point-of-care bacterial detection FL-imaging feature was employed in a prospective longitudinal study involving 30 patients to assess its effectiveness in monitoring and managing PIs. These data are further contextualized with the results of a post-hoc analysis of clinical trial1 data from 22 PIs comparing the device's bacterial detection sensitivity against SOC. Lastly, a case series of at-risk patients where thermal imaging highlighted findings on pressure points in relation to possible DTIs, and in some cases, the enhancement of inflammation/infection detection through thermal imaging.
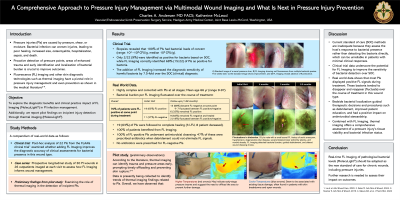
Results: In the prospective study, most patients had a single active PI, primarily located in the ischial (39%) and sacral/coccygeal (45%) areas. Positive FL signals were found in 70% of PIs, leading to modified treatment plans (e.g., more/new debridement, antibiotics, etc.) in 58% of visits. Continuous monitoring showed fluctuating bacterial loads in 30% of cases. Biopsies confirmed all PIs had concerning bacterial loads, but standard assessments only detected 10% as positive for clinical signs of infection; FL imaging increased detection to 64%. In a few cases where thermal imaging was used concurrently with FL-imaging, our understanding of the extent of wound-associated cellulitis was enhanced. None of the PIs developed complications (e.g. osteomyelitis, sepsis) and all progressed positively without requiring hospitalization. Thermal imaging showed warmer areas indicating early-stage DTI, while lower temperatures correlated with clinically visible tissue damage.
Discussion: Integrating thermal and FL-imaging into pressure injury management enhances prevention and treatment at all stages. Thermal imaging assesses skin damage and DTI risk, FL-imaging (+/- Thermal) helps ascertain infection, and thermal imaging helps evaluate recurrence risk after healing. This approach improves outcomes, reduces healthcare burdens, and may lower liability and costs.

.jpg)