
.jpg)
Case Series/Study
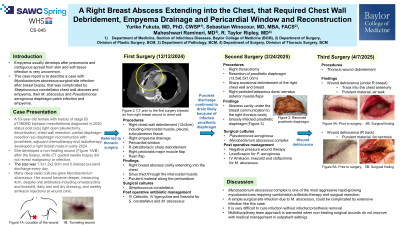
Empyema usually develops after pneumonia and contiguous spread from skin and soft tissue infection is very uncommon. The aim of this report is to describe a case with Mycobacterium abscessus surgical site infection after breast biopsy, that was complicated by Streptococcus constellatus chest wall abscess and empyema
Methods:
Results:
Case:
A 53-year-old female with history of stage IB pT3N0M0 biphasic mesothelioma s/p right open pleurectomy, decortication, chest wall resection, adjuvant chemotherapy and radiotherapy, developed a right breast mass. Although CT guided needle biopsy did not reveal malignancy or infection, she developed a non-healing wound after the biopsy. The size was 1.3x1.2x2.9cm and it drained purulent discharge every day. Many deep swab cultures grew Mycobacterium abscessus. Her wound became deeper, measuring 4cm, despite oral antibiotics including omadacycline and linezolid, daily wet and dry dressing, and weekly amikacin injections at wound clinic. CT chest only showed pleurodesis changes about the right hemithorax with extensive atelectasis of the right lung. Incision and exploratory evaluation in the operating room was performed by thoracic surgery in conjunction with plastic surgery. The chest wall had purulent material that was draining through a sinus tract in the intercostal muscle. The area was opened and purulent material drained from the intrathoracic cavity along the pericardium. The intercostal muscle, the residual thoracic cavity, the subcutaneous fat and the chest wall were debrided. Pericardium window was performed. Right pectoralis major muscle flap and Ryan flap were performed by plastic surgery. Multiple surgical cultures grew Streptococcus constellatus. The histopathology showed granulation tissue and scarring, negative for malignancy. Special stains for Gomori Methenamine-Silver Nitrate and Acid Fast Bacteria were negative for fungal and acid-fast micro-organisms. Acid Fast Bacteria cultures have been negative for 3 weeks so far. She was discharged with outpatient parental antibiotics including cefoxitin and tigecycline along with oral linezolid.
Discussion:
This is the first case Mycobacterium abscessus surgical site infection was complicated by Streptococcus constellatus chest wall abscess and empyema. Mycobacterium abscessus complex is one of the most aggressive rapid-growing mycobacterium requiring combination antibiotic therapy and surgical resection. A simple non-healing wound could be complicated by extensive infection. Multidisciplinary team approach is warranted when non-healing surgical wounds do not improve with medical management in outpatient settings.