
.jpg)
Evidence-Based Practice
Current best practices of wound care focus on healing as early as possible which includes making a correct diagnosis, recognizing the red flags that impede wound healing, and initiating early intervention acknowledging that chronicity is not time dependent. Initial wound evaluations are often performed first by urgent care, emergency responders, or primary care professionals who are skilled in their field but are not chronic wound specialists. These medical providers are often unfamiliar with current wound care scoring systems that aid in determining wound severity, guiding early interventions, and identifying the need for specialized care based on patients’ overall medical condition and the wound status. A referral to a wound specialist has the potential to expedite healing, reduce overall cost of care, alleviate patient suffering, and ultimately save a limb or life.
Methods:
The BIOMES scoring scale is a tool that serves as a method to quickly assess wounds as moderate to high risk for being hard-to-heal. The acronym BIOMES provides the front-line clinicians who perform initial patient assessments with succinct direction in the early identification of barriers to healing of moderate- to high-risk wounds. Each letter guides the clinician to evaluate a part of the patient’s medical history or wound presentation that may affect the healing trajectory.
Results:
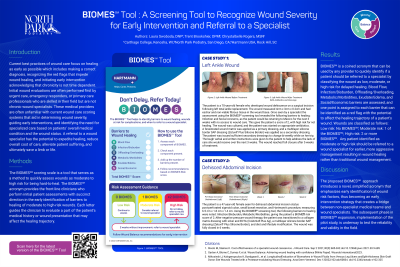
BIOMES is a generic acronym that can be used by any provider to quickly identify if a patient should be referred to a specialist by classifying the wound as low, moderate, or high risk for delayed healing. Blood Flow, Infection/Bioburden, Offloading/Overloading, Metabolic/Morbidities, Exudate/Edema, and Social/Economic barriers are assessed, and one point is assigned to each barrier that can be identified as a red flag with the potential to affect the healing trajectory of a patient’s wound. Wounds are classified as follows: Low risk: No BIOMES; Moderate risk: 1 of the BIOMES; High risk: 2 or more BIOMES. Any patient identified as moderate or high risk should be referred to a wound specialist for earlier, more aggressive management resulting in wound healing rather than traditional wound management.
Discussion:
The proposed BIOMES approach introduces a novel simplified acronym that emphasizes early identification of wound risk factors, thus becoming an early intervention strategy that creates a bridge between non-specialist medical teams and wound specialists. The subsequent phase in BIOMES expansion, implementation of the pilot study, is underway to test the reliability and validity in the field.