(CS-115) Improving Wound Hygiene Through Fluorescence Imaging: A Focus on Spatial Patterns in Diabetic and Venous Leg Ulcers
Friday, May 2, 2025
7:45 PM - 8:45 PM East Coast USA Time
Amit Rao, MD – Northwell Health; Farisha Baksh, BS – Northwell Health; Sally Kaplan, RN – Northwell Health
Introduction: Wound cleansing, performed at every wound care appointment, is necessary to put stalled wounds back onto a healing trajectory and to prevent infection and its complications. The advent of bacterial fluorescence imaging technology* for wound care has changed our understanding of bacterial distribution in wounds and allows us to evaluate wound hygiene efficacy in real-time. Clinical studies using fluorescence imaging show that significant bacterial colonization is frequently left behind following standard cleansing practices1, highlighting the potential for improvement.
Methods: We present a clinical algorithm for effective wound hygiene informed by real-time fluorescence imaging of bacteria and biofilm. Clinical cases illustrate this approach and demonstrate consistent spatial patterns of bacterial fluorescence in venous leg ulcers (VLUs) and diabetic foot ulcers (DFUs). We also discuss practical insights obtained from our routine use of fluorescence imaging that will improve wound hygiene practices for clinicians without access to this technology.
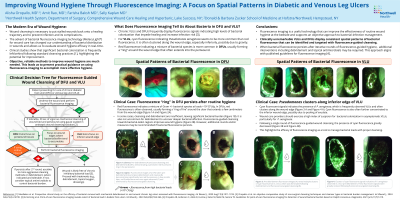
Results: Clinically unremarkable VLUs and DFUs frequently display fluorescence signals indicating high levels of bacterial colonization. For VLUs, cyan fluorescence indicating Pseudomonas aeruginosa is often clustered along the inferior wound edge. Red fluorescence indicating a mixture of bacterial species is more common in DFUs, usually forming a “ring” around the ulcer that extends a few centimeters from the wound edge. We recommend fluorescence imaging before and after wound cleansing, and that providers use fluorescence signals to guide cleansing towards bacterial-laden regions. In cases where bacterial fluorescence cannot be removed after a single round of guided hygiene, we recommend additional rounds and/or additional measures such as debridement and topical antimicrobials. This approach aligns with published guidelines for fluorescence imaging3 and has led to improved healing outcomes in clinical studies4.
Discussion: Wound care providers should exercise a high index of suspicion for bacterial colonization in asymptomatic wounds, and particularly for P. aeruginosa in VLUs. Areas of focus for wound cleansing may differ between VLUs and DFUs, however thorough hygiene across the entire wound bed and periwound is always recommended. Fluorescence imaging is useful for guiding wound cleansing, for confirming its efficacy, and for assessing the need for additional measures such as debridement or antimicrobials.

.jpg)