(PI-044) The Use of a Multilayered Leukocyte, Platelet and Fibrin Patch in Conjunction with Near-infrared Spectroscopy for Difficult to Heal Diabetic Foot Ulcers
Friday, May 2, 2025
7:45 PM - 8:45 PM East Coast USA Time
Lucy Gachimu, RN – Program Director, Wound Center, St. Vincent Hospital, Worcester, MA
Introduction: Diabetic foot ulcers (DFU) continue to be challenging to treat appropriately, and the costs associated continue to grow. One statistic is that one million dollars are spent on diabetic foot complications every 30 minutes in the US. As health care providers, it is imperative that the interventions chosen for DFU are effective and evidence based. The multilayered leukocyte, platelet, and fibrin patch (MLPF) has been proven to accelerate wound healing in DFU, even in patients with low ankle-brachial indices (ABI). However, the ABI is no longer considered the gold standard to determine ischemia. Near-Infrared Spectroscopy (NIRS) is a new diagnostic tool that allows providers to determine if wounds are adequately perfused, which is essential to wound healing. The ability to provide a high concentration of the patient’s own blood cells to an ischemic wound is a novel concept provided by the MLPF patch. This study sought to determine if providing an MLPF patch to a proven ischemic DFU using NIRS would have positive outcomes.
Methods: Our center uses NIRS before and after debridement to determine if adequate debridement has been performed and if adequate perfusion is present. We have adopted this process when applying the MLPF patch to ensure proper wound bed preparation and positive outcomes in ischemic wounds.
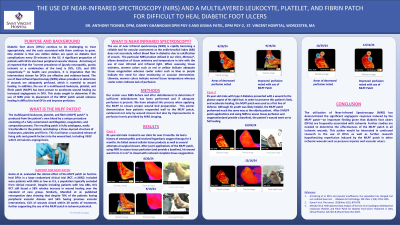
Results: We have treated numerous patients with the MLPF patch in conjunction with NIRS to ensure adequate tissue perfusion.One example of a successful outcome was an 81-year-old male had been treated in our clinic for 10 months. He had a history of osteomyelitis and had been receiving hyperbaric oxygen therapy with little healing noted. Also, different cellular tissue products and surgical closures were tried to no avail. After just six applications of the MLPF patch, along with the use of NIRS, his wound healed from an initial measurement of 5.3 cm2.
Discussion: The use of NIRS has been quickly gaining adoption among wound care providers as a better option to determine perfusion than the ankle-brachial index and other similar diagnostics. With the use of NIRS, a provider can determine if adequate perfusion is present in a wound, therefore allowing better wound bed preparation for advanced therapies. When used with NIRS, the multilayered leukocyte, platelet and fibrin patch has improved healing and outcomes in chronic diabetic wounds. More research is needed to determine the effectiveness of the MLPF patch on confirmed ischemic wounds without the presence of diabetes.

.jpg)