(CS-088) Using a Multilayered Leukocyte Platelet Fibrin Patch over Exposed Bone and Tendon: A Case Series
Friday, May 2, 2025
7:45 PM - 8:45 PM East Coast USA Time
Tiffany Keith, PA-C
Introduction: Healing chronic wounds is particularly challenging when an exposed structure such as bone or tendon is presentdue to poor vascularization surrounding these structures. When comorbidities and limited complianceare also a factor, the wound is at increased risk of infection with approximately 20% of patients with diabetic foot ulcers (DFUs) developing osteomyelitis. Early advanced modalities combined with good standard of care can greatly improve the time to heal.The use of a multilayered leukocyte, platelet, fibrin p</span>atch (MLPF) is one therapy that shows promise in this patient population, where few options are available.
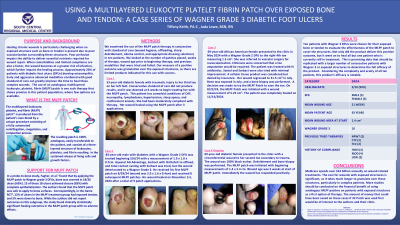
Methods: We examined MLPF patch therapy with standard of care (wound hygiene, offloading, sharp debridement, edema control, and appropriate dressing selection) in several patients.We looked at the number of patches placed, weeks of therapy, wound age prior to therapy, and previously used modalities. The desired outcome wasgranulation over the exposed structures, as there are limited indicated products.
Results: One 84-year-oldmalehad a Wagner Grade 2 DFU measuring 1.9 x 1.8 x 0.7cm first treated on 5/6/24. Several dressings and offloading was tried, but the wound deteriorated to a Wagner Grade 3. He received his first MLPF patch on 8/29/24 and received 8 subsequentMLPF patches with healing achieved on November 1st, 2024. An 86-year-old male with a DFU, treated osteomyelitis, and bone exposurefailedto progress for over 6 months. The patient received his first MLPF patch on 8/14/24 and after 3 patches, combined with total contact casting, the patient healed. Lastly, a69-year-old femalepresented to the clinic in May 2024 with a right 4th toe Wagner Grade 2 DFU measuring 1.5 cm2. She was referred for revascularization due to possible need for toe amputation. The patient was treated with IV antibiotics as well as other products with minimal improvement. A cellular tissue product was considered but denied by insurance.Her wound regressed to 31.5 cm2 in July with bone exposed;a bone was biopsied. The MLPF Patch was started in an attempt to save the toe on 8/22/24.Thepatientwas completelyhealed on 11/13/2024.
Discussion: Medicare spends over $32 billion annually on wound relatedtreatments. The cost for wounds with exposed structures is significant, as it takes much longer to granulate over these structures. More studies should be conducted on the financial benefit of using autologous MLPF patches on patients with exposed structures as a first option of therapy.

.jpg)