(CS-040) Percutaneous Double Bypass in Setting of Non-healing Chronic Ulcer for Lower Extremity Revascularization
Friday, May 2, 2025
7:45 PM - 8:45 PM East Coast USA Time
Kanu Alieu, DPM; Nicholas Petruzzi, MD; Talia Younus, DPM
Introduction: Atherosclerosis affecting the lower extremities frequently results in rest pain, non-healing ulcers and extensive soft tissue loss. Peripheral arterial disease affects 8-10 million people in the USA (3). It is characterized by atherosclerotic occlusions that can occur in any of the arteries of the lower extremity and limit blood flow to one or both lower extremities. For patients with non-healing ulcers, re-establishing flow to the area facilitates healing. The angiosome concept (AC) introduced in 1987 by Taylor and Palmer divided the body into three-dimensional vascular territories supplied by specific source arteries (4). According to the AC, the foot and ankle has six distinct angiosomes arising from the posterior tibial artery, anterior tibial artery, and peroneal artery. Revascularization based on the angiosome concept is highly debatable for various reasons but has been used successfully. Open bypass and endovascular bypass techniques have been the mainstay of revascularization. Endovascular bypass has several advantages over open, including decreased recovery time and wound infections. With modern advancements in endovascular medicine, the DETOUR bypass has become frontline therapy for long segment SFA disease. In our case, the patient had a previous endovascular bypass (popliteal to posterior tibial) but developed a non-healing ulcer with cellulitis in the anterior tibial angiosome requiring revascularization that was performed using DETOUR bypass.
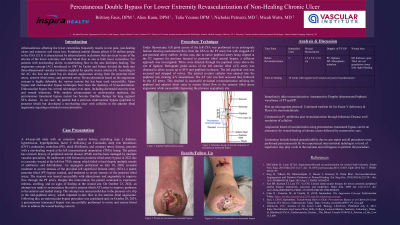
Methods: Wires were directed through the popliteal artery above the site of ligation. The left anterior tibial (AT) artery was accessed. The left popliteal vein was accessed and stripped of valves. The arterial popliteal re-entry catheter was entered into the popliteal vein. Through pedal retrograde access the AT vein was accessed followed by the AT artery. This resulted in successful endoluminal bypass utilizing the popliteal and anterior tibial veins to restore blood flow to the anterior tibial artery angiosome.
Results: To date, the wound on the left lower extremity post revascularization has decreased significantly in size with a granular wound base.
Discussion: Angiosome based revascularization using the DETOUR bypass can be an alternative therapy for wound healing of non-healing ulcers in a specific angiosome followed by conservative care.

.jpg)