(PI-031) Lessening Limb Loss with Interstate Collaboration in Charcot Arthropathy and Osteomyelitis
Friday, May 2, 2025
7:45 PM - 8:45 PM East Coast USA Time
Brock Liden, DPM – Surgical Services, Berger Health System, Circleville, OH, United States
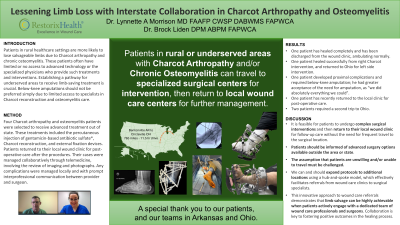
Introduction: Patients in rural healthcare settings are more likely to lose salvageable limbs due to Charcot arthropathy and chronic osteomyelitis. These patients often have limited or no access to advanced technology or the specialized physicians who provide such treatments and interventions. Establishing a pathway for underserved areas to receive limb-saving treatment is crucial. Below-knee amputations should not be preferred simply due to limited access to specialists in Charcot reconstruction and osteomyelitis care.
Methods: Four Charcot arthropathy and osteomyelitis patients were selected to receive advanced treatment out of state. These treatments included the percutaneous injection of gentamicin-based antibiotic sulfate*, Charcot reconstruction, and external fixation devices. Patients returned to their local wound clinic for post-operative care after the procedures. Their cases were managed collaboratively through telemedicine, involving the review of imaging and photographs. Any complications were managed locally and with prompt interprofessional communication between provider and surgeon.
*Trade marked- Cerament G
Results: Two patients have healed, are walking and have been discharged from the wound care clinic, one patient developed proximal complications and will unfortunately require below-knee amputation, and one patient has recently returned to the local clinic for post-operative care. One patient required a second trip to the surgical location; the remainder of patients have been managed in the local area.
Discussion: It is feasible for patients to undergo complex surgical interventions and then return to their local wound clinic for follow-up care without the need for frequent travel to the surgical location. Patients should be informed of advanced surgery options available outside the area or state. As evidenced here, the assumption that patients are unwilling and/or unable to travel must be challenged. We can and should expand protocols to additional locations using a hub-and-spoke model, which effectively facilitates referrals from wound care clinics to surgical specialists. This innovative approach to wound care referrals demonstrates that limb salvage can be highly achievable when patients actively engage with a dedicated team of wound care professionals and surgeons. Collaboration is key to fostering positive outcomes in the healing process.

.jpg)