
.jpg)
Case Series/Study
Chronic ulcerations in diabetic patients with foot deformities present significant challenges, particularly when compounded by osteomyelitis and biomechanical abnormalities. Equinovarus contractures worsen pressure points, leading to non-healing wounds. Standard wound care and offloading often fail in these cases, necessitating surgical intervention. This report highlights a multimodal approach combining tendon releases, deformity correction, dead space management with piscine graft, and external fixation to achieve wound closure and restore function.
Methods:
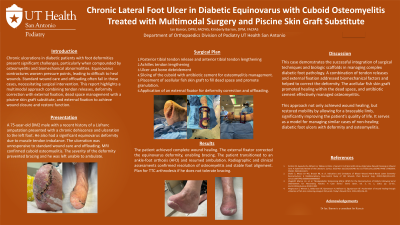
A 75-year-old diabetic male with a history of Lisfranc amputation presented with a chronic lateral foot ulcer secondary to equinovarus deformity. The ulceration was unresponsive to standard wound care and offloading. MRI confirmed cuboid osteomyelitis, and the deformity prevented bracing and functional ambulation. Surgical intervention included:
The patient achieved complete wound healing. The external fixator corrected the equinovarus deformity, enabling bracing. The patient transitioned to an ankle-foot orthosis (AFO) and resumed ambulation. Radiographic and clinical assessments confirmed resolution of osteomyelitis and stable foot alignment.
Discussion:
This case demonstrates the successful integration of surgical techniques and biologic scaffolds in managing complex diabetic foot pathology. Tendon releases and Achilles lengthening addressed biomechanical factors, while the external fixator corrected deformity, enabling mobility. The acellular fish skin graft promoted healing within the dead space, and antibiotic cement effectively managed osteomyelitis.
This approach not only achieved wound healing but restored functional mobility, significantly improving the patient’s quality of life. It serves as a model for managing similar cases of non-healing diabetic foot ulcers with deformity and osteomyelitis.