
.jpg)
Case Series/Study
Symmetric peripheral gangrene (SPG) is characterized by peripheral ischemic lesions without significant vascular occlusion. SPG mortality rates range from 40% to 90%. SPG manifests as peripheral cyanosis, mottling, and symmetrical ischemia in the distal limbs, which can lead to gangrene. Although the underlying etiology is not quite understood, the pathophysiology has been tied to three main factors: disseminated intravascular coagulation (DIC), use of vasopressors, and microbiological influences. Management strategies focus on addressing the underlying conditions, with wound care customized to the specific clinical scenario. This case details a patient found to have SPG whose wound care was adapted to his clinical presentation.
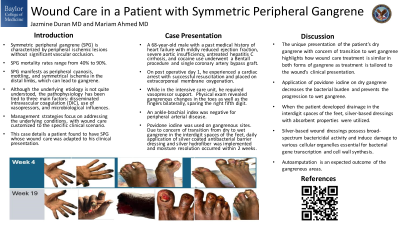
A 68-year-old male with a past medical history of heart failure with mildly reduced ejection fraction, severe aortic insufficiency, untreated hepatitis C cirrhosis, and cocaine use underwent a Bentall procedure and single coronary artery bypass graft. On post operative day 1, he experienced a cardiac arrest with successful resuscitation and placed on extracorporeal membrane oxygenation. While in the intensive care unit, he required vasopressor support. Physical exam revealed gangrenous changes in the toes as well as the fingers bilaterally, sparing the right fifth digit. An ankle-brachial index was negative for peripheral arterial disease. Povidone iodine was used on gangrenous sites. Due to concern of transition from dry to wet gangrene in the interdigit spaces of the feet, daily application of silver coated antibacterial barrier dressing and silver hydrofiber was implemented and moisture resolution occurred within 2 weeks.
Methods:
Results:
Discussion:
The unique presentation of the patient’s dry gangrene with concern of transition to wet gangrene highlights how wound care treatment is similar in both forms of gangrene as treatment is tailored to the wound’s clinical presentation. Application of povidone iodine on dry gangrene decreases the bacterial burden and prevents the progression to wet gangrene. When the patient developed drainage in the interdigit spaces of the feet, silver-based dressings with absorbent properties were utilized. Silver-based wound dressings possess broad-spectrum bactericidal activity and induce damage to various cellular organelles essential for bacterial gene transcription and cell wall synthesis. Autoamputation is an expected outcome of the gangrenous areas.